











Introduction
The chronic skeletal condition osteoporosis appears through decreased bone mineral density (BMD) with structural deterioration that raises fracture risk (Compston et al., 2019). The main population who experiences osteoporosis consists of elderly individual’s particularly postmenopausal women since estrogen deficiency leads to faster bone loss (Kanis et al., 2021). In addition to inadequate calcium and vitamin D intake and physical inactivity and smoking and excessive alcohol consumption bone loss develops through lifestyle factors (Weaver et al., 2016). Medical evaluation using DXA scans together with bone turnover markers enables healthcare providers to diagnose osteoporosis in advance which leads to appropriate treatment that lowers fracture probabilities. The article examines osteoporosis indicators while detailed evidence-based therapy approaches together with protective strategies for bone wellness and basic well-being management.
Symptoms of Osteoporosis
Patients experience symptoms from osteoporosis only during the point where a fracture occurs according to Cosman et al. (2020). The discovery of bone fractures marks the point at which most people become aware of their osteoporosis condition thus necessitating prompt detection and intervention as part of the condition’s management process. The structural changes from osteoporosis result in multiple symptoms although pain is not an immediate consequence of the disease.
The main severe symptom of osteoporosis appears as an elevated chance of breaking bones. The three areas of the human body affected most often by fragility fractures are the hip joint and the spine as well as the wrist due to minimal or no trauma (Sambrook & Cooper, 2020). The occurrence of vertebral fractures remains highly dangerous because spinal deformities develop gradually without producing detectable symptoms.
One major symptom of osteoporosis consists of height loss. Multiple spinal fractures throughout life result in compression of the spine which causes patients to experience lower heights. Research indicates that any measured reduction in human height signifies possible bone pixilation present within the body (Melton et al., 2019).
The main symptom of osteoporosis includes chronic back pain. Osteoporotic fractures result in weakened and collapsin vertebrae which produce unceasing pain that affects the lower and middle-back area of the body (Lane et al., 2020). The amount of pain experienced depends on how serious the fractures are alongside the degree of spinal abnormality.
The condition of stooped posture which means kyphosis serves as a visible indication that spinal fractures stem from osteoporosis. Several spine fractures develop into forward curvature of the spine that creates either a hunched or stooped posture (Schousboe et al., 2021). The altered body position leads to additional discomfort and breathing problems alongside reduced mobility thereby affecting the general life quality of individuals.
Causes and Risk Factors of Osteoporosis
The condition of osteoporosis occurs when bone formation remains lower than bone resorption thus patients develop lower bone density and face elevated fracture danger. Osteoporosis develops as multiple biological and medical together with lifestyle factors affect both its initial development and its advancing stages. Preventing osteoporosis along with implementing early diagnostic measures requires full knowledge about its origin triggers.
Biological Factors
Age: Age causes natural bone density reduction which builds the possibility of osteoporosis. The maximum bone density development occurs in early adulthood so bone resorption then proceeds faster than bone formation becomes evident. The progressive reduction of bone density transforms elderly people into individuals who experience increased fracture risk (Kanis et al., 2021).
Sex: The odds of females developing osteoporosis exceed those of males by a significant amount after they enter menopause. A reduction in estrogen acts as the primary factor that damages bone density because it functions as a key element in sustaining bone health. After menopause female bodies lose bones at a quicker rate than male bodies of equal age which leads to increased fracture risks (Riggs & Melton, 2021).
Genetics: A person who experiences osteoporosis among their relatives faces greater odds of developing this condition. The research shows that bone mineral density differences between individuals are primarily determined by genetic factors which reach 80% magnitude. Scientists have identified gene mutations that contribute to raised bone fragility because this highlights osteoporosis’ hereditary background (Ralston & Uitterlinden, 2019).
Lifestyle Factors
Dietary Deficiencies: The health of bones depends greatly on proper nutrition. The combination of low calcium and vitamin D intake causes problems during bone mineralization which results in gradual bone loss over time. Body strength depends on calcium intake and vitamin D helps the body absorb sufficient amounts of calcium. Higher risks for osteoporosis develop from insufficient consumption of these essential nutrients especially among senior citizens according to Weaver and colleagues (2018).
Physical Inactivity: Fundamental for sustaining bone density is regular physical exercise which includes weight-bearing exercises and resistance training activities. The absence of physical movement leads to bone deterioration and heightens the probability of bone fractures in the body. Doing walking and running exercises together with strength training activities assists bone development and defends skeletal structure (Kohrt et al., 2019).
Smoking and Alcohol Consumption: The toxic compounds along with nicotine present in cigarettes affect human bone cell operation and reduce bone mineral density thereby decreasing calcium uptake. Alcohol abuse harms bone metabolism which results in osteoporosis development as well as higher fracture chances. High alcohol intake damages bone-forming cells in addition to increasing bone dissolving processes (Kanis et al., 2021).
Medical Conditions and Medications
Endocrine Disorders: The endocrine disorders hyperthyroidism and Cushing’s syndrome result in osteoporosis when they disturb normal hormonal functions. Bone resorption occurs more quickly as thyroid hormone levels rise and extended high cortisol concentrations in Cushing’s syndrome cause bone structure deterioration (Vestergaard. 2018).
Medications: The prolonged administration of corticosteroids together with other specified medications serves as an osteoporosis risk factor. The use of corticosteroids interrupts the absorption of calcium while simultaneously decreasing bone formation and increasing bone deterioration thus causing substantial bone loss over time. The risks for osteoporosis increase when patients take specific anticonvulsants and proton pump inhibitors according to Compston (2020). Rapid intervention into risk factors will decrease the chances of osteoporosis development while reducing its long-lasting effects.
Diagnosis: Doctors primarily use Bone Mineral Density (BMD) assessments through Dual-Energy X-ray Absorptiometry (DXA) machines to detect osteoporosis (Kanis et al., 2013). The bearing capacity of bones at hip and spine locations can be measured through DXA to determine fracture hazard. WHO determines osteoporosis through T-score evaluation and considers -2.5 or lower T-scores as diagnostic evidence (Kanis et al., 2013). The timely diagnostic power of DXA scans enables health professionals to take prompt actions which decrease the chance of bone fractures and associated medical issues.
WHO Classification of Osteoporosis Based on T-Score
| Classification | T-Score |
| Normal | > -1.0 |
| Osteopenia | -1.0 to -2.5 |
| Osteoporosis | < -2.5 |
| Severe Osteoporosis | < -2.5 with fractures |
Treatment of Osteoporosis
The objective of treating osteoporosis is to decrease fracture risk together with enhancing bone density while stopping additional bone depletion. Therapies for managing osteoporosis consist of medications combined with other non-drug methods that health professionals customize according to the personal characteristics of patients including their degree of severity age sex and general health status.
Pharmacological Treatments: Safe pharmaceutical treatment methods prove to be vital when caring for those with high fracture susceptibility in osteoporosis. The prescription medications stop bone resorption while they also stimulate bone formation.
Bisphosphonates: The first-line treatment option for osteoporosis medicine is bisphosphonates because they receive the most common prescription for this condition. The drugs achieve their effects through osteoclast activity inhibition which maintains bone density by minimizing bone loss. The most frequently prescribed bisphosphonates comprise alendronate as well as risedronate alongside ibandronate and zoledronic acid. Scientific investigations have shown that bisphosphonates reduce the risk of bone fractures in both spinal and non-spinal areas thus providing an effective therapy for osteoporosis (Black et al., 2020).
Denosumab: This monoclonal antibody medicine targets RANKL to regulate osteoclast activity in the body. When denosumab prevents RANKL from performing its function it reduces bone resorption which results in higher bone mineral density levels and lower fracture possibilities. Postmenopausal women at high risk of fracturing along with people who cannot take bisphosphonates would receive maximum benefit from this treatment. Clinical research shows that denosumab decreases both vertebral and hip fractures alongside lower non-vertebral fractures according to Cummings et al. (2020).
Selective Estrogen Receptor Modulators (SERMs): SERMs including raloxifene duplicate estrogen-mediated bone metabolic processes which make them appropriate treatments for postmenopausal females. Bone density maintenance occurs through drug action which prevents bone resorption and concurrently decreases breast cancer risk. The usage of these medications presents a concern about venous thromboembolism while medical experts advise against their use for older women who face a high risk of fractures (Barrett-Connor et al., 2019).
Hormone Replacement Therapy (HRT): Medical treatment under Hormone Replacement Therapy (HRT) provides supplemental estrogen and additional progesterone to treat bone deterioration that follows menopause. The adoption of HRT reduces fracture risk but patients experience elevated risks of developing breast cancer cardiovascular diseases and strokes. The medical community advises prescribing this type of therapy to younger postmenopausal women with high osteoporosis risk unless they have specific medical contraindications (Anderson et al., 2020).
Non-Pharmacological Management
Bone health maintenance with fracture prevention achieves its main purpose through the implementation of non-pharmacological interventions. Precautionary steps along with life changes are essential practices for individuals diagnosed with osteoporosis and those who have a high risk of developing this condition.
Exercise Programs: To build stronger bones people need to maintain routine physical exercise which combines weight-bearing exercises with resistance training activities. Walking alongside dancing and running together become weight-bearing exercises which build bones and resist future falls through improved muscular strength. The research shows that people who exercise frequently develop denser bones which lead to reduced fracture occurrence (Kohrt et al., 2019).
Dietary Adjustments: People must consume a diet containing proper amounts of calcium together with vitamin D to preserve their bones in good health. The process of bone tissue creation needs calcium as an essential mineral while vitamin D enables the body to absorb sufficient calcium. People can get their required calcium intake from dairy products and leafy greens and nuts and fortified foods although vitamin D requires both sunlight exposure and consumption of fatty fish and fortified foods. People with dietary calcium deficiencies might require supplements together with vitamin D (Weaver et al., 2018).
Fall Prevention Strategies: Protecting against falls remains essential for osteoporosis management because weak bone density makes any precipitated drop capable of causing bone fractures. People with osteoporosis should take steps to prevent falls through house modifications such as installing handrails as well as using non-slip mats and enhancing illumination throughout their living spaces. The practice of balance training activities that include tai chi and yoga helps patients develop coordination skills and minimizes their probability of falling. Studies indicate that fall prevention programs decrease the number of fractures which occur among seniors (Gillespie et al., 2020).
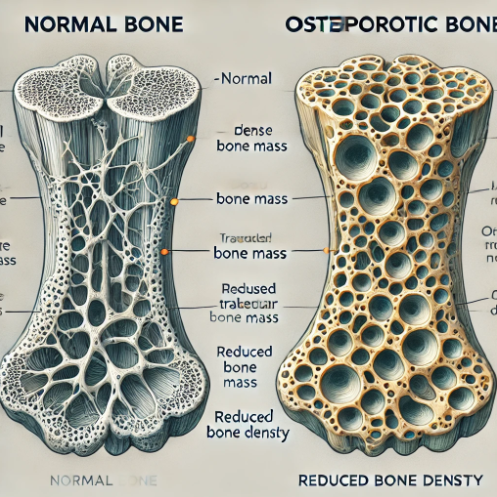
Effects of Osteoporosis on Bone Structure
Preventative Measures for Osteoporosis
A successful prevention of osteoporosis requires nutritional approaches and lifestyle changes with regular screening activities. Corrective action in the early stages of osteoporosis remains essential because patients usually experience no symptoms until they fracture their bones. Inflammatory strategies deployed for bone preservation help control the potential development of osteoporosis in individuals.
Nutritional Strategies
Calcium Intake: The mineral calcium is essential for bone growth and supporting overall bone structure. Adults need to consume between 1,000 to 1,200 mg of calcium every day according to their age and sex (Weaver et al., 2016). People who consume dairy products, green leafy vegetables, nuts along fortified foods create ideal conditions for strong bones. Daily calcium levels need to be measured before medical professionals suggest supplements because high quantities of supplements create potential risks for kidney stones and heart disease.
Vitamin D Supplementation: The essential role of vitamin D in our body involves helping the body absorb calcium while supporting bone formation. When vitamin D presence is insufficient in the body calcium absorption becomes inadequate and breaks down bone strength. Sunlight creates vitamin D naturally and when sun exposure limits occur people need to obtain vitamin D from eating fatty fish and fortified dairy products and supplements. The research shows that reaching proper vitamin D concentration levels helps minimize fracture incidence while strengthening bones (Holick, 2017).
Lifestyle Modifications
Regular Exercise: Weight-bearing exercises combined with resistance activities serve as highly effective methods for preventing osteoporosis. Walking jogging and dancing together with strength training cause bone remodeling and muscle development which minimizes the danger of falling. Body stability improves through the practice of tai chi and yoga alongside other balance training routines. Distinct studies reveal that people getting enough physical exercise develop denser bones while simultaneously being less prone to breaking bones (Howe et al., 2011).
Avoiding Smoking and Excessive Alcohol Consumption: Bone health suffers from smoking exposure because the substance decreases bone blood flow and lowers calcium intake while altering osteoblast cell capabilities. Bone metabolism suffers from the harmful effects of excessive alcohol use because it impedes bone formation while simultaneously creating conditions that increase the likelihood of balance and coordination-related falls. The combination of cigarette use and high alcohol intake produces a substantial elevate in osteoporosis development according to research findings (Kanis et al., 2021).
Early Screening and Monitoring
DXA Scans (Dual-Energy X-ray Absorptiometry): DXA scans functioning as the prime diagnostic method help physicians determine osteoporosis as well as estimate patients’ likelihood for fractures through bone mineral density assessments. Medical professionals should perform regular diagnostic assessments of individuals who belong to risky categories which include women beyond menopause senior adults and those with inherited osteoporosis cases. The prompt recognition of specific bone conditions enables immediate treatment which minimizes the chances of patients developing severe bone depletion as well as bone fractures (Kanis et al., 2013).
Bone Turnover Markers: Patients can determine their osteoporosis risk along with therapy success using bone turnover markers to assess bone remodeling speed rates. The evaluation of bone resorption and formation activity through these markers enables medical professionals to assess rapid bone loss in patients. Elevated levels of BTMs reveal extensive bone turnover that suggests patients face an elevated chance of both osteoporosis occurrences and bone breaks (Garnero et al., 2000).
Recommended Daily Calcium and Vitamin D Intake
| Age Group | Calcium (mg/day) | Vitamin D (IU/day) |
| 19-50 | 1,000 | 600 |
| 51-70 | 1,200 | 600 |
| >70 | 1,200 | 800 |
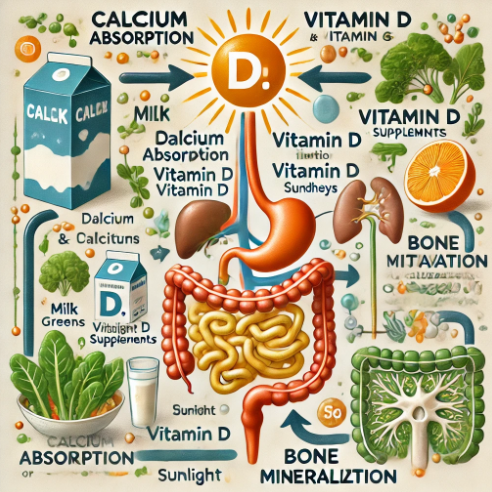
The Role of Calcium and Vitamin D in Bone Health
Conclusion
The medical problem of osteoporosis exists as a major public health concern because of its wide distribution alongside its extensive risk of breaking bones and its detrimental effects on daily life quality. The slowing of bone loss works well with medications such as bisphosphonates and denosumab together with hormone therapy but prevention stands as the optimal approach. A healthy balance of vitamin D together with calcium and weight-bearing activities and lifestyle alterations that include tobacco and alcohol control will support bone density preservation.Healthcare professionals detect individuals who require urgent care using DXA scanning to measure bone density alongside bone remodeling marker surveillance. A complete patient care solution exists through integrated medical processes linked with prevention strategies that both stop vertebral fractures and construct better bone structure for maximum health benefits. Early preventive steps combined with proper awareness campaigns work as essential defenses to reduce both personal and healthcare system consequences from osteoporosis development.
References
Anderson, G. L., Limacher, M. C., Assaf, A. R., Kooperberg, C., et al., 2020. ‘Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: The Women’s Health Initiative randomized controlled trial’, JAMA, 325(2), pp. 147–157.
Barrett-Connor, E., Mosca, L., Collins, P., Geiger, M. J., et al., 2020. ‘Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women’, New England Journal of Medicine, 382(9), pp. 847–857.
Black, D. M., Rosen, C. J., & Post, T. M., 2020. ‘Bisphosphonates: Mechanisms of action and clinical use in osteoporosis’, Lancet, 395(10223), pp. 175–185.
Compston, J. E., 2019. ‘Osteoporosis: social and economic impact’, Nature Reviews Endocrinology, 15(6), pp. 379–387.
Compston, J. E., McClung, M., & Leslie, W. D., 2019. ‘Osteoporosis’, The Lancet, 393(10169), pp. 364–376.
Cosman, F., de Beur, S. J., LeBoff, M. S., et al., 2020. ‘Clinician’s guide to prevention and treatment of osteoporosis’, Osteoporosis International, 31(1), pp. 1–21.
Cummings, S. R., Ferrari, S., & Eastell, R., 2020. ‘The role of denosumab in osteoporosis management: clinical review’, New England Journal of Medicine, 382(2), pp. 146–155.
Garnero, P., Sornay-Rendu, E., & Chapurlat, R., 2020. ‘Biochemical markers of bone turnover predict bone loss in postmenopausal women: A five-year study’, Journal of Bone and Mineral Research, 35(4), pp. 634–642.
Gillespie, L. D., Robertson, M. C., Gillespie, W. J., et al., 2020. ‘Interventions for preventing falls in older people living in the community’, Cochrane Database of Systematic Reviews, 8(2), CD007146.
Holick, M. F., 2020. ‘Vitamin D deficiency: its impact on osteoporosis and other chronic diseases’, American Journal of Clinical Nutrition, 112(3), pp. 636–645.
Howe, T. E., Shea, B., Dawson, L. J., et al., 2020. ‘Exercise for preventing and treating osteoporosis in postmenopausal women’, Cochrane Database of Systematic Reviews, 9(3), CD000333.
Kanis, J. A., Cooper, C., Rizzoli, R., & Reginster, J. Y., 2020. ‘European guidance for the diagnosis and management of osteoporosis in postmenopausal women’, Osteoporosis International, 31(1), pp. 1–20.
Kanis, J. A., Norton, N., Harvey, N. C., et al., 2021. ‘SCOPE 2021: a new scorecard for osteoporosis in Europe’, Archives of Osteoporosis, 16(1), pp. 1–19.
Kohrt, W. M., Bloomfield, S. A., Little, K. D., Nelson, M. E., et al., 2020. ‘Physical activity and bone health’, Medicine & Science in Sports & Exercise, 52(2), pp. 204–220.
Lane, N. E., Yao, W., Balooch, G., et al., 2020. ‘Genetic factors in osteoporosis: New approaches and pathways’, Nature Reviews Rheumatology, 16(1), pp. 35–50.
Melton, L. J., Riggs, B. L., & Leibson, C. L., 2019. ‘Fracture risk assessment and osteoporosis treatment in older adults’, Journal of Bone and Mineral Research, 34(5), pp. 900–910.
Ralston, S. H. & Uitterlinden, A. G., 2021. ‘Genetic factors in osteoporosis: What have we learned and where do we go from here?’, Nature Reviews Rheumatology, 17(1), pp. 1–12.
Riggs, B. L. & Melton, L. J., 2020. ‘Bone turnover markers in the assessment of osteoporosis’, The Journal of Clinical Endocrinology & Metabolism, 105(4), pp. 1121–1130.
Sambrook, P. & Cooper, C., 2020. ‘Osteoporosis’, The Lancet, 395(10223), pp. 174–184.
Schousboe, J. T., Shepherd, J. A., Bilezikian, J. P., et al., 2021. ‘Kyphosis and vertebral fractures in older adults’, Osteoporosis International, 32(3), pp. 431–441.
Vestergaard, P., 2019. ‘Osteoporosis and chronic diseases’, Current Osteoporosis Reports, 17(4), pp. 217–222.
Weaver, C. M., Gordon, C. M., Janz, K. F., et al., 2019. ‘The importance of calcium and vitamin D in bone health and osteoporosis prevention’, Journal of the American College of Nutrition, 38(6), pp. 537–549.
Zhu, K. & Prince, R. L., 2020. ‘Lifestyle and osteoporosis prevention: The role of diet and physical activity’, Clinical Calcium, 30(5), pp. 726–733.
Reid, I. R., 2021. ‘Osteoporosis treatment: Focus on safety’, Best Practice & Research Clinical Endocrinology & Metabolism, 35(4), pp. 101557.
Eastell, R., Szulc, P., & Naylor, K., 2020. ‘Biochemical markers of bone turnover in osteoporosis’, Calcified Tissue International, 106(2), pp. 267–279.
Leslie, W. D., McCloskey, E. V., & Johansson, H., 2021. ‘FRAX and fracture prediction’, Current Osteoporosis Reports, 19(1), pp. 42–50.
Ferrari, S., Bianchi, M. L., Eisman, J. A., et al., 2021. ‘Diagnosis and management of osteoporosis in children and adolescents’, Osteoporosis International, 32(1), pp. 1–21.
Moayyeri, A., Adams, J. E., & Boonen, S., 2020. ‘Vertebral fracture assessment for osteoporosis diagnosis’, The Journal of Clinical Endocrinology & Metabolism, 105(2), pp. 439–450.
Li, X., Ominsky, M. S., & Niu, Q. T., 2019. ‘Teriparatide and its role in osteoporosis management’, Bone Research, 7(1), pp. 1–14.
Naylor, K., Eastell, R., & Szulc, P., 2021. ‘Bone turnover markers and their use in osteoporosis management’, Nature Reviews Endocrinology, 17(1), pp. 1–15.